
December 3 is International Day of Persons with Disabilities Day. I knew I wanted to do a blog post honoring this day since I work with individuals of all abilities, however, I was stumped on the best way to do this. Then a friend sent me this amazing video from the New York City Marathon. Kayleigh Williamson became one of the first women to run a marathon with Down Syndrome at the NYC Marathon. If you haven’t seen it, you need to check it out. It gives me chills every time I watch it. It also reminded me how exercise can look different for each person.
This is one of the things I love about being a PT. We help individualize rehabilitation programs that include exercise for each person. When looking at the research, it was also noted that people living with disabilities are up to 62% less likely to meet physical activity guidelines than people without disabilities. So this brings up the question and fear, is it safe to exercise? There are many factors to consider, so it is important to consult your medical team and local physical therapist prior to starting a program. But the short answer is typically YES, but modifications are often needed. This is the importance of finding a provider that is familiar or willing to research and understand the cause and development of your diagnosis. First, lets define exercise.
Exercise is “planned, structured, and repetitive exercises with an increasing magnitude and intensity in order to maintain or improve physical fitness or aerobic capacity.”
It is important to note that exercise is different from physical activity. Physical activity is what we do throughout the day, while exercise is more planned and repetitive. Physical activity is any movement and exercise is a type of physical activity.
Common goals that exercise can address are the following:
- Maximize function
- Minimize contracture
- Decrease weight gain
- Decrease rate of deterioration
- Maintain bone strength
When building a new program, starting with the FITT principle is a great place to start.

Frequency and Time – The American College of Sports Medicine (ACSM) is our gold standard when recommending exercise. They recommend 60 minutes per day in the 6-18 year age range. Phew, that sounds like a lot! But this is a goal and something that can and should be built up to. This is where the intensity and type are important so we can meet each person at their level. People living with disabilities can even achieve benefits if under this time threshold!
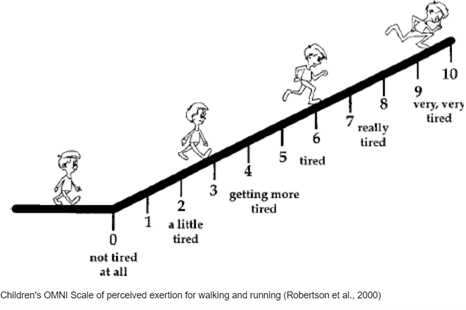
Intensity – How hard are we working. The goal is usually moderate intensity. There are a couple techniques to figure this out, but I want to highlight Rating Perceived Exertion (RPE) or Omni Scale. This is a numerical scale of how hard you feel like you are working. The talk test is another way to do this. You should be able to keep steady conversation while in the moderate zone. My moderate will be different than yours! These scales are great because it is individualized and easy to use.
Type – How do we exercise. This can be done through a combination of strengthening, stretching, and aerobic activities. There are many different techniques of exercises that you can complete.

- Aerobic: This is getting your heart rate up. Kayleigh was a great example of this by completing a full marathon. But not all aerobic needs to look like running. Two other examples are adapted/non adapted bike riding and aquatic therapy/swimming.

- Strengthening: This can be done through body weight only or with the use of resistance. If moving your arms and legs against gravity is difficult, the aquatic environment and Slings and Springs are great options. Slings and Springs is shown in the picture here. You will need a set up that is sturdy enough to support your arm or leg. The picture is a demonstration of a handmade PVC set up while working on leg strength.
- Flexibility: Contractures, or decreased range of motion at a joint, is common among many diagnoses. Even slight contractures can impact your function. Muscle weakness and muscle tone can impact our ability to have full flexibility. Stretching with the assist of a caregiver or completed by yourself are different ways to help maintain or slow contracture rate.
Okay this is where I get a little nerdy (eek, check out that reference list). But I wanted to take a look at the research for some diagnosis specific examples for you. Lets see what I found:
- Cerebral Palsy (CP): Benefits are noted at even a reduced dose of frequency and intensity.
- Down Syndrome: Leg strength, balance, bone strength, and heart health can be improved with a resistance program.
- Duchenne Muscular Dystrophy: “The No Use is Disuse study” has shown low intensity physical training is safe and can delay deterioration
- Spinal Muscular Atrophy (SMA): Individuals can achieve the ACSM guidelines when modified and slowly progressed within 6 months without being harmful.
- Cancer: Exercise can help decrease cancer related comorbidities and has been noted to be safe and effective even during the most aggressive phases
I wanted to close out on a study that highlights the importance of keeping it fun. Exercise Intensity During Power Wheelchair Soccer” included children and adults with diagnoses of CP, SMA, spinal cord injury, and muscular dystrophies. They found that intensity is increased with power wheelchair soccer. This is important because we want to find fun ways to incorporate exercise daily, especially with our kids. This is an age appropriate-activity and can include peers!
In conclusion, exercise may look different depending on factors in your lifestyle. We still need more evidence for specific guidelines since research protocols do vary, but we do know it appears to be safe when done correctly. For it to be impactful, keep it fun and part of your regular routine. Hang in there, effects are mostly seen with long term duration. What is your favorite way to exercise? Drop a comment below if I missed one of your exercise techniques.
If you need help developing an exercise program, a physical therapy comprehensive evaluation could be right for you.
Alternate Links
To see Kayleigh Williamson’s beautiful NYC Marathon finish on Instagram, click here.
To see it on Facebook, use this link.
References
2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, 2018.
Jansen M, van Alfen N, Geurts AC, et al. Assisted bicycle training delays functional deterioration in boys with duchenne muscular dystrophy: the randomized controlled trial “no use is disuse”. Neurorehabil Neural Repair 2013;27:816-27.
Salazar R, Montes J, Dunaway Young S, McDermott MP, Martens W, Pasternak A, et al. Quantitative evaluation of lower extremity joint contractures in spinal muscular atrophy: implications for motor function. Pediatr Phys Ther. 2018;30(3):209–15. https://doi.org/10.1097/PEP.0000000000000515.
Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Heal Rep 1985;100:126-31
Voet, N (2019). Exercise in Neuromuscular Disorders: A Promising Intervention. ACTA Myologica 38 ($): 207-214
Toldi, James DO; Escobar, Joseph MD; Brown, Austin MD. Cerebral Palsy: Sport and Exercise Considerations. Current Sports Medicine Reports 20(1):p 19-25, January 2021. | DOI: 10.1249/JSR.0000000000000798
Paul Y, Ellapen TJ, Barnard M, Hammill HV, Swanepoel M. The health benefits of exercise therapy for patients with Down syndrome: A systematic review. Afr J Disabil. 2019 Oct 23;8:576. doi: 10.4102/ajod.v8i0.576. PMID: 31745461; PMCID: PMC6852506.
Melo GLR, Neto IVS, da Fonseca EF, Stone W, Nascimento DDC. Resistance training and Down Syndrome: A narrative review on considerations for exercise prescription and safety. Front Physiol. 2022 Sep 27;13:948439. doi: 10.3389/fphys.2022.948439. PMID: 36237528; PMCID: PMC9553130.
Morales JS, Valenzuela PL, Velázquez-Díaz D, Castillo-García A, Jiménez-Pavón D, Lucia A, Fiuza-Luces C. Exercise and Childhood Cancer-A Historical Review. Cancers (Basel). 2021 Dec 24;14(1):82. doi: 10.3390/cancers14010082. PMID: 35008246; PMCID: PMC8750946.
Bartels B, Montes J, van der Pol WL, de Groot JF. Physical exercise training for type 3 spinal muscular atrophy. Cochrane Database Syst Rev. 2019 Mar 1;3(3):CD012120. doi: 10.1002/14651858.CD012120.pub2. PMID: 30821348; PMCID: PMC6396106.
Barfield JP, Newsome L, Malone LA. Exercise Intensity During Power Wheelchair Soccer. Arch Phys Med Rehabil. 2016 Nov;97(11):1938-1944. doi: 10.1016/j.apmr.2016.05.012. Epub 2016 Jun 8. PMID: 27288710.
Melo GLR, Neto IVS, da Fonseca EF, Stone W, Nascimento DDC. Resistance training and Down Syndrome: A narrative review on considerations for exercise prescription and safety. Front Physiol. 2022 Sep 27;13:948439. doi: 10.3389/fphys.2022.948439. PMID: 36237528; PMCID: PMC9553130.
Ginis K. a. M., Van Der Ploeg H. P., Foster C., Lai B., Mcbride C. B., Ng K., et al. (2021). Participation of people living with disabilities in physical activity: A global perspective. Lancet 398, 443–455. 10.1016/S0140-6736(21)01164-8

Leave a Reply